The Silent Crisis: How Sarcoidosis Highlights the Urgent Need for Biomedical Equity
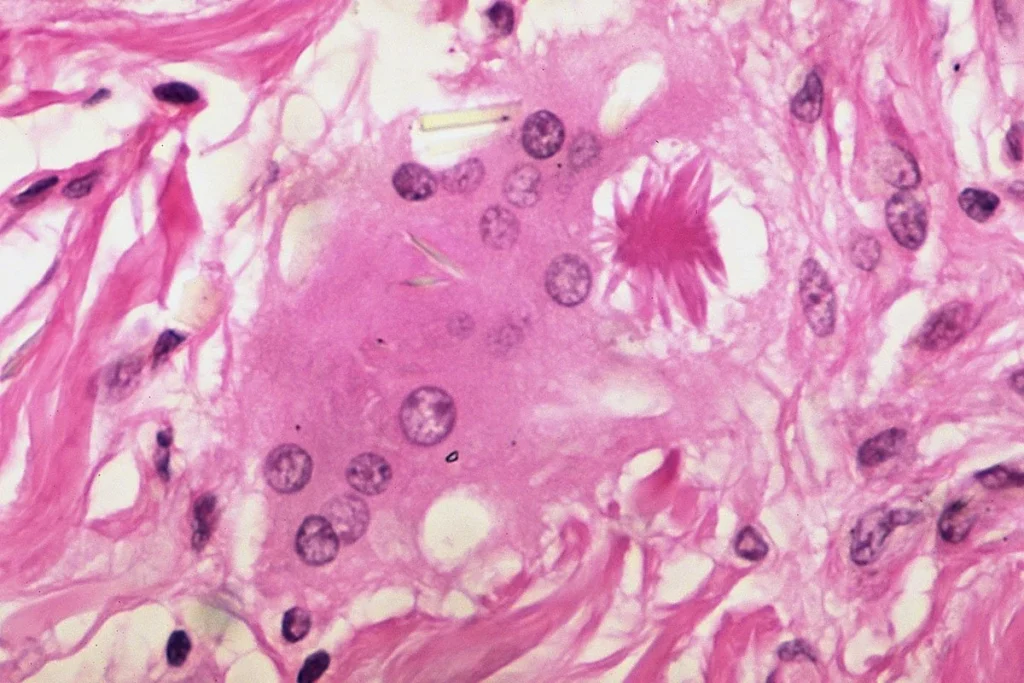
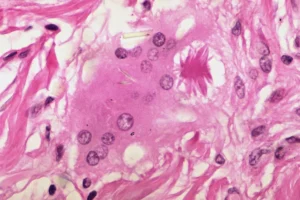
Sarcoidosis, a rare and often debilitating inflammatory disease, has long occupied the shadows of medical research. Characterized by the growth of tiny collections of inflammatory cells—known as granulomas—in different parts of the body, the disease remains a diagnostic enigma. While it can affect any organ, it most commonly targets the lungs and lymph nodes, leading to a spectrum of symptoms ranging from mild fatigue and joint pain to life-threatening heart rhythm disturbances and irreversible organ damage.
Beyond the biological complexity, sarcoidosis serves as a stark prism through which the systemic inequities of the American healthcare system are refracted. The disease disproportionately ravages Black American communities, particularly Black women, yet these same populations are consistently sidelined in clinical trials and medical research. As philanthropic organizations like the Milken Institute and the Ann Theodore Foundation begin to pioneer new funding models, the medical community is forced to confront a uncomfortable reality: without equity, we are not just failing patients—we are failing science itself.
The Anatomy of an Invisible Disease
Sarcoidosis is an "orphan disease," meaning it lacks the broad public awareness and robust research funding often afforded to more common conditions. Affecting approximately 150,000 to 200,000 people in the United States, its etiology remains unknown. Because the disease manifests differently in every patient, it is notoriously difficult to diagnose.
For many, the journey to a diagnosis is a multi-year odyssey of misdiagnosis, medical gaslighting, and mounting frustration. Because common symptoms—such as fatigue, brain fog, and muscle aches—are often dismissed as non-specific, patients frequently cycle through specialists before receiving an accurate diagnosis. Even when identified, the therapeutic arsenal is severely limited. Standard treatments, such as corticosteroids and harsh chemotherapeutics, are designed to suppress the immune system to mitigate symptoms, but they do nothing to reverse the underlying pathology and often carry their own heavy burden of side effects.
A History of Disproportionate Impact
The burden of sarcoidosis is not distributed equally. Epidemiological data paints a harrowing picture of racial disparity:
- Prevalence: Black Americans are 2.2 to 5.6 times more likely to be diagnosed with sarcoidosis than their White, Hispanic, or Asian counterparts.
- The Gender Gap: Black women experience the highest prevalence of any demographic, with rates double those of Black men and up to six times those of White, Asian, and Hispanic women.
- Severity: Clinical outcomes are consistently poorer for Black patients, who tend to experience more severe, organ-threatening forms of the disease.
Despite this clear epidemiological evidence, Black patients remain severely underrepresented in clinical research. Data indicates that Black participation in interstitial lung disease trials—which encompass sarcoidosis—hovers at a dismal 5 percent. This lack of representation creates a dangerous feedback loop: clinical trials are designed for a demographic that does not reflect the actual population suffering from the disease, leading to treatments that may not be optimized for the very people who need them most.
Chronology of a Systemic Failure
To understand why the current research landscape for sarcoidosis is so fractured, one must look at the historical trajectory of the American biomedical ecosystem.
The Era of Exclusion (Mid-20th Century)
Historically, clinical research was largely conducted within white-centric academic medical centers, with little regard for the diversity of the patient population. Practices like the Tuskegee Syphilis Study left a deep, well-earned scar of distrust between the Black community and the medical establishment—a mistrust that persists to this day and is often cited by patients as a barrier to participating in modern clinical trials.
The Rise of Underfunding (1980s–2010s)
As federal research funding became increasingly competitive, rare diseases were often relegated to the back of the queue. Sarcoidosis, lacking a powerful lobby or widespread awareness, suffered from decades of stagnant investment. During this period, the "medical divide" widened, as research infrastructure became concentrated in elite, predominantly white institutions, further distancing the scientific community from the populations most impacted by the disease.
The Modern Reckoning (2020–Present)
The dual crises of the COVID-19 pandemic and the renewed focus on systemic racism following the 2020 social justice movements forced a reckoning within the medical industry. Organizations like the Foundation for Sarcoidosis Research (FSR) began conducting deep-dive surveys into patient experiences. The results were clear: the barriers were not merely biological; they were logistical, financial, and psychological. Patients cited a lack of information about trials, fears regarding safety, and insurmountable logistical costs—such as the inability to take time off work or find childcare—as primary reasons for non-participation.
Supporting Data: The Pipeline Problem
The lack of diversity in clinical trials is mirrored by a lack of diversity in the professional ranks of medicine. As of 2018, only 5 percent of practicing physicians in the United States were Black. This is not an accident; it is the result of a long-standing failure to build and sustain pipelines for Black medical professionals.
The infrastructure gap is perhaps most evident in the underfunding of Historically Black Colleges and Universities (HBCUs). While HBCUs represent only 2.3 percent of U.S. medical schools, they have historically produced nearly 70 percent of the nation’s Black physicians and dentists. Yet, these institutions are systematically starved of the research capital necessary to compete with R1 universities. In 2023, the cumulative research funding for all HBCUs combined was less than one-fifth of the funding awarded to a single institution, Johns Hopkins. This resource disparity prevents Black researchers from leading the studies that could solve health crises within their own communities.
The Role of Philanthropy: A New Model of Intervention
In the face of government bureaucracy and the slow churn of federal grant-making, private philanthropy is emerging as a vital, agile actor. The partnership between the Milken Institute and the Ann Theodore Foundation offers a blueprint for the future. By dedicating over half a million dollars to a clinical trial for an existing, FDA-approved therapeutic that shows promise for sarcoidosis, these organizations are bypassing the "red tape" that often stalls life-saving innovation.
This model is significant for three reasons:
- Speed: It prioritizes immediate, actionable research over long-term, high-risk exploration.
- Flexibility: It allows for funding that covers not just the science, but the logistical support needed to make participation possible for patients, such as transportation and compensation for lost wages.
- Targeting: It focuses on diseases that have been neglected by traditional market-driven pharmaceutical investment.
Implications for the Future of Medicine
The lessons learned from the sarcoidosis crisis have profound implications for the broader biomedical field. If medicine continues to operate on a "one-size-fits-all" model, it will continue to perpetuate health inequities.
Investing in HBCUs
The most promising path toward systemic change lies in bolstering HBCU research infrastructure. By providing stable, long-term funding to these institutions, philanthropy can help bridge the gap in the scientific workforce, ensuring that the next generation of researchers includes individuals with the lived experience and cultural competency to address diseases that have historically been ignored.
Building Trust Through Transparency
The medical establishment must reckon with the fact that trust is not given; it is earned. Building a more inclusive research environment requires radical transparency. This means not only inviting diverse patient populations to participate in trials but involving them in the design of those trials. It means acknowledging the historical harms of the medical system and actively working to dismantle the power structures that exclude Black, Hispanic, and Indigenous communities from the conversation.
The Necessity of Holistic Funding
Finally, the sarcoidosis case study proves that scientific breakthroughs cannot be separated from the socio-economic context of the patient. Research funding must evolve to include "social determinants of health" in its scope. A drug is only effective if it can be accessed; a trial is only valid if the population is representative.
Conclusion: A Call for Coordinated Action
Sarcoidosis is a disease that demands a systemic response. The progress made by the Milken Institute and the Ann Theodore Foundation is a crucial first step, but it is not a panacea. The goal must be to move beyond isolated, project-based interventions and toward a fundamental redesign of the research ecosystem.
Whether one is a philanthropist, a policymaker, or a researcher, the imperative is the same: science must be inclusive to be accurate. When we ignore the communities most burdened by disease, we do not just perpetuate injustice—we limit the scope of our own medical potential. By investing in the institutions that serve these communities and prioritizing the voices of those who have been historically silenced, we can finally begin to turn the tide against sarcoidosis and the wider landscape of health disparities. The science of the future must be built on a foundation of equity, or it will remain an incomplete endeavor.